Heel Pains The Causes, Indicators And Therapy Methods
Overview

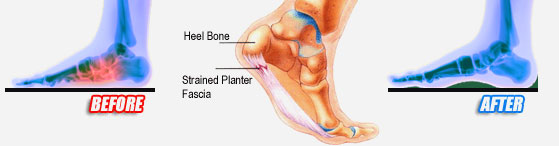
Heel pain is a very common foot problem. The sufferer usually feels pain either under the heel (planter fasciitis) or just behind it (Achilles tendinitis), where the Achilles tendon connects to the heel bone. Even though heel pain can be severe and sometimes disabling, it is rarely a health threat. Heel pain is typically mild and usually disappears on its own; however, in some cases the pain may persist and become chronic (long-term). There are 26 bones in the human foot, of which the heel (calcaneus) is the largest. The human heel is designed to provide a rigid support for the weight of the body. When we are walking or running it absorbs the impact of the foot when it hits the ground, and springs us forward into our next stride. Experts say that the stress placed on a foot when walking may be 1.25 times our body weight, and 2.75 times when running. Consequently, the heel is vulnerable to damage, and ultimately pain.
Causes
Long standing inflammation causes the deposition of calcium at the point where the plantar fascia inserts into the heel. This results in the appearance of a sharp thorn like heel spur on x-ray. The heel spur is asymptomatic (not painful), the pain arises from the inflammation of the plantar fascia.
Symptoms
The symptoms of plantar fasciitis are classically pain of a sharp nature which is worse standing first thing in the morning. After a short period of walking the pain usually reduces or disappears, only to return again later in the day. Aggravating times are often after increased activity and rising from sitting. If these are the sort of symptoms you are experiencing then the Heel-Fix Kit ? will be just the treatment your heel is crying out for. Some heel pain is more noticeable at night and at rest. Because plantar fasciitis is a mechanical pathology it is unlikely that this sort of heel pain is caused by plantar fasciitis. The most common reason for night heel pain is pressure on your Sciatic nerve causing referred pain in the heel. Back pain is often present as well, but you can get the heel pain with little or no back pain that is caused by nerve irritation in the leg or back. If you get pain in your heels mainly or worse at night please see a clinician as soon as you can to confirm the diagnosis.
Diagnosis
In most cases, your GP or a podiatrist (a specialist in foot problems and foot care) should be able to diagnose the cause of your heel pain by asking about your symptoms and medical history, examining your heel and foot.
Non Surgical Treatment
If pain and other symptoms of inflammation-redness, swelling, heat-persist, you should limit normal daily activities and contact our office, or another doctor of podiatric medicine. Your foot would be examined, and an X-ray may be taken to rule out problems of the bone. Early treatment might involve oral or injectable anti-inflammatory medication, taping, padding, massage, stretching, exercise, shoe recommendations, physiotherapy, over-the-counter shoe inserts or, if the condition is chronic and there is a biomechanical basis to the complaint, orthoses (or orthotic devices) may be used to permanently take strain off the fascia. Only rarely is surgery required for heel pain. If necessary, however, it may involve the release of the plantar fascia, removal of a spur, removal of a bursa, or removal of a neuroma or other soft-tissue growth.
Surgical Treatment
When a diagnosis of plantar fasciitis is made early, most patients respond to conservative treatment and don?t require surgical intervention. Often, when there is a secondary diagnosis contributing to your pain, such as an entrapped nerve, and you are non-responsive to conservative care, surgery may be considered. Dr. Talarico will discuss all options and which approach would be the most beneficial for your condition.
what does a heel spur look like
Prevention
Flexibility is key when it comes to staving off the pain associated with these heel conditions. The body is designed to work in harmony, so stretching shouldn?t be concentrated solely on the foot itself. The sympathetic tendons and muscles that move the foot should also be stretched and gently exercised to ensure the best results for your heel stretches. Take the time to stretch thighs, calves and ankles to encourage healthy blood flow and relaxed muscle tension that will keep pain to a minimum. If ice is recommended by a doctor, try freezing a half bottle of water and slowly rolling your bare foot back and forth over it for as long as is comfortable. The use of elastic or canvas straps to facilitate stretching of an extended leg can also be helpful when stretching without an assistant handy. Once cleared by a doctor, a daily regimen of over-the-counter anti-inflammatory medication like Naproxen Sodium will keep pain at bay and increase flexibility in those afflicted by heel pain. While this medication is not intended to act as a substitute for medical assessments, orthopedics or stretching, it can nonetheless be helpful in keeping discomfort muted enough to enjoy daily life. When taking any medication for your heel pain, be sure to follow directions regarding food and drink, and ask your pharmacist about possible interactions with existing medications or frequent activities.
Heel pain is a very common foot problem. The sufferer usually feels pain either under the heel (planter fasciitis) or just behind it (Achilles tendinitis), where the Achilles tendon connects to the heel bone. Even though heel pain can be severe and sometimes disabling, it is rarely a health threat. Heel pain is typically mild and usually disappears on its own; however, in some cases the pain may persist and become chronic (long-term). There are 26 bones in the human foot, of which the heel (calcaneus) is the largest. The human heel is designed to provide a rigid support for the weight of the body. When we are walking or running it absorbs the impact of the foot when it hits the ground, and springs us forward into our next stride. Experts say that the stress placed on a foot when walking may be 1.25 times our body weight, and 2.75 times when running. Consequently, the heel is vulnerable to damage, and ultimately pain.
Causes
Long standing inflammation causes the deposition of calcium at the point where the plantar fascia inserts into the heel. This results in the appearance of a sharp thorn like heel spur on x-ray. The heel spur is asymptomatic (not painful), the pain arises from the inflammation of the plantar fascia.
Symptoms
The symptoms of plantar fasciitis are classically pain of a sharp nature which is worse standing first thing in the morning. After a short period of walking the pain usually reduces or disappears, only to return again later in the day. Aggravating times are often after increased activity and rising from sitting. If these are the sort of symptoms you are experiencing then the Heel-Fix Kit ? will be just the treatment your heel is crying out for. Some heel pain is more noticeable at night and at rest. Because plantar fasciitis is a mechanical pathology it is unlikely that this sort of heel pain is caused by plantar fasciitis. The most common reason for night heel pain is pressure on your Sciatic nerve causing referred pain in the heel. Back pain is often present as well, but you can get the heel pain with little or no back pain that is caused by nerve irritation in the leg or back. If you get pain in your heels mainly or worse at night please see a clinician as soon as you can to confirm the diagnosis.
Diagnosis
In most cases, your GP or a podiatrist (a specialist in foot problems and foot care) should be able to diagnose the cause of your heel pain by asking about your symptoms and medical history, examining your heel and foot.
Non Surgical Treatment
If pain and other symptoms of inflammation-redness, swelling, heat-persist, you should limit normal daily activities and contact our office, or another doctor of podiatric medicine. Your foot would be examined, and an X-ray may be taken to rule out problems of the bone. Early treatment might involve oral or injectable anti-inflammatory medication, taping, padding, massage, stretching, exercise, shoe recommendations, physiotherapy, over-the-counter shoe inserts or, if the condition is chronic and there is a biomechanical basis to the complaint, orthoses (or orthotic devices) may be used to permanently take strain off the fascia. Only rarely is surgery required for heel pain. If necessary, however, it may involve the release of the plantar fascia, removal of a spur, removal of a bursa, or removal of a neuroma or other soft-tissue growth.
Surgical Treatment
When a diagnosis of plantar fasciitis is made early, most patients respond to conservative treatment and don?t require surgical intervention. Often, when there is a secondary diagnosis contributing to your pain, such as an entrapped nerve, and you are non-responsive to conservative care, surgery may be considered. Dr. Talarico will discuss all options and which approach would be the most beneficial for your condition.
what does a heel spur look like
Prevention
Flexibility is key when it comes to staving off the pain associated with these heel conditions. The body is designed to work in harmony, so stretching shouldn?t be concentrated solely on the foot itself. The sympathetic tendons and muscles that move the foot should also be stretched and gently exercised to ensure the best results for your heel stretches. Take the time to stretch thighs, calves and ankles to encourage healthy blood flow and relaxed muscle tension that will keep pain to a minimum. If ice is recommended by a doctor, try freezing a half bottle of water and slowly rolling your bare foot back and forth over it for as long as is comfortable. The use of elastic or canvas straps to facilitate stretching of an extended leg can also be helpful when stretching without an assistant handy. Once cleared by a doctor, a daily regimen of over-the-counter anti-inflammatory medication like Naproxen Sodium will keep pain at bay and increase flexibility in those afflicted by heel pain. While this medication is not intended to act as a substitute for medical assessments, orthopedics or stretching, it can nonetheless be helpful in keeping discomfort muted enough to enjoy daily life. When taking any medication for your heel pain, be sure to follow directions regarding food and drink, and ask your pharmacist about possible interactions with existing medications or frequent activities.
Exercises To Improve Leg Length Discrepancy
Overview
Many people undergo surgery for various reasons - arthritis, knee replacement, hip replacement, even back surgery. However, the underlying cause of leg length inequality still remains. So after expensive and painful surgery, follow by time-consuming and painful rehab, the true culprit still remains. Resuming normal activities only continues to place undue stress on the already overloaded side. Sadly so, years down the road more surgeries are recommended for other joints that now endure the excessive forces.
Causes
Leg length discrepancies can be caused by poor alignment of the pelvis or simply because one leg is structurally longer than the other. Regardless of the reason, your body wants to be symmetrical and will do its best to compensate for the length difference. The greater the leg length difference, the earlier the symptoms will present themselves to the patient. Specific diagnoses that coincide with leg length discrepancy include: scoliosis, lumbar herniated discs, sacroiliitis, pelvic obiliquity, greater trochanteric bursitis, hip arthritis, piriformis syndrome, patellofemoral syndrome and foot pronation. Other potential causes could be due to an injury (such as a fracture), bone disease, bone tumors, congenital problems (present at birth) or from a neuromuscular problem.
Symptoms
LLD do not have any pain or discomfort directly associated with the difference of one leg over the other leg. However, LLD will place stress on joints throughout the skeletal structure of the body and create discomfort as a byproduct of the LLD. Just as it is normal for your feet to vary slightly in size, a mild difference in leg length is normal, too. A more pronounced LLD, however, can create abnormalities when walking or running and adversely affect healthy balance and posture. Symptoms include a slight limp. Walking can even become stressful, requiring more effort and energy. Sometimes knee pain, hip pain and lower back pain develop. Foot mechanics are also affected causing a variety of complications in the foot, not the least, over pronating, metatarsalgia, bunions, hammer toes, instep pain, posterior tibial tendonitis, and many more.
Diagnosis
Asymmetry is a clue that a LLD is present. The center of gravity will shift to the short limb side and patients will try to compensate, displaying indications such as pelvic tilt, lumbar scoliosis, knee flexion, or unilateral foot pronation. Asking simple questions such as, "Do you favor one leg over the other?" or, "Do you find it uncomfortable to stand?" may also provide some valuable information. Performing a gait analysis will yield some clues as to how the patient compensates during ambulation. Using plantar pressure plates can indicate load pressure differences between the feet. It is helpful if the gait analysis can be video-recorded and played back in slow motion to catch the subtle aspects of movement.
Non Surgical Treatment
A properly made foot orthotic can go a long way in substituting additional millimeters or centimeter on the deficient side. Additional full length inserts are added to the shorter side bringing the runner closer to symmetrical. Heel lifts do not work in runners because when you run you may land on your heel but the rest of the time you are on your forefoot then your toes pushing off. The right custom-made, biomechanical orthotic can address the underlying cause of your pain. Abnormal joint position, overpronation or foot rigidity can be addressed and the biomechanics normalized. San Diego Running Institute orthotics are custom molded to your foot and are designed with your specific body weight, leg length discrepancy, and activity in mind. The restoration of correct mechanical function takes the abnormal stress from the uneven side and allows the body to heal naturally.

shoe lift inserts
Surgical Treatment
Shortening techniques can be used after skeletal maturity to achieve leg length equality. Shortening can be done in the proximal femur using a blade plate or hip screw, in the mid-diaphysis of the femur using a closed intramedullary (IM) technique, or in the tibia. Shortening is an accurate technique and involves a much shorter convalescence than lengthening techniques. Quadriceps weakness may occur with femoral shortenings, especially if a mid-diaphyseal shortening of greater than 10% is done. If the femoral shortening is done proximally, no significant weakness should result. Tibial shortening can be done, but there may be a residual bulkiness to the leg, and risks of nonunion and compartment syndrome are higher. If a tibial shortening is done, shortening over an IM nail and prophylactic compartment release are recommended. We limit the use of shortenings to 4 to 5 cm leg length inequality in patients who are skeletally mature.
Many people undergo surgery for various reasons - arthritis, knee replacement, hip replacement, even back surgery. However, the underlying cause of leg length inequality still remains. So after expensive and painful surgery, follow by time-consuming and painful rehab, the true culprit still remains. Resuming normal activities only continues to place undue stress on the already overloaded side. Sadly so, years down the road more surgeries are recommended for other joints that now endure the excessive forces.
Causes
Leg length discrepancies can be caused by poor alignment of the pelvis or simply because one leg is structurally longer than the other. Regardless of the reason, your body wants to be symmetrical and will do its best to compensate for the length difference. The greater the leg length difference, the earlier the symptoms will present themselves to the patient. Specific diagnoses that coincide with leg length discrepancy include: scoliosis, lumbar herniated discs, sacroiliitis, pelvic obiliquity, greater trochanteric bursitis, hip arthritis, piriformis syndrome, patellofemoral syndrome and foot pronation. Other potential causes could be due to an injury (such as a fracture), bone disease, bone tumors, congenital problems (present at birth) or from a neuromuscular problem.
Symptoms
LLD do not have any pain or discomfort directly associated with the difference of one leg over the other leg. However, LLD will place stress on joints throughout the skeletal structure of the body and create discomfort as a byproduct of the LLD. Just as it is normal for your feet to vary slightly in size, a mild difference in leg length is normal, too. A more pronounced LLD, however, can create abnormalities when walking or running and adversely affect healthy balance and posture. Symptoms include a slight limp. Walking can even become stressful, requiring more effort and energy. Sometimes knee pain, hip pain and lower back pain develop. Foot mechanics are also affected causing a variety of complications in the foot, not the least, over pronating, metatarsalgia, bunions, hammer toes, instep pain, posterior tibial tendonitis, and many more.
Diagnosis
Asymmetry is a clue that a LLD is present. The center of gravity will shift to the short limb side and patients will try to compensate, displaying indications such as pelvic tilt, lumbar scoliosis, knee flexion, or unilateral foot pronation. Asking simple questions such as, "Do you favor one leg over the other?" or, "Do you find it uncomfortable to stand?" may also provide some valuable information. Performing a gait analysis will yield some clues as to how the patient compensates during ambulation. Using plantar pressure plates can indicate load pressure differences between the feet. It is helpful if the gait analysis can be video-recorded and played back in slow motion to catch the subtle aspects of movement.
Non Surgical Treatment
A properly made foot orthotic can go a long way in substituting additional millimeters or centimeter on the deficient side. Additional full length inserts are added to the shorter side bringing the runner closer to symmetrical. Heel lifts do not work in runners because when you run you may land on your heel but the rest of the time you are on your forefoot then your toes pushing off. The right custom-made, biomechanical orthotic can address the underlying cause of your pain. Abnormal joint position, overpronation or foot rigidity can be addressed and the biomechanics normalized. San Diego Running Institute orthotics are custom molded to your foot and are designed with your specific body weight, leg length discrepancy, and activity in mind. The restoration of correct mechanical function takes the abnormal stress from the uneven side and allows the body to heal naturally.
shoe lift inserts
Surgical Treatment
Shortening techniques can be used after skeletal maturity to achieve leg length equality. Shortening can be done in the proximal femur using a blade plate or hip screw, in the mid-diaphysis of the femur using a closed intramedullary (IM) technique, or in the tibia. Shortening is an accurate technique and involves a much shorter convalescence than lengthening techniques. Quadriceps weakness may occur with femoral shortenings, especially if a mid-diaphyseal shortening of greater than 10% is done. If the femoral shortening is done proximally, no significant weakness should result. Tibial shortening can be done, but there may be a residual bulkiness to the leg, and risks of nonunion and compartment syndrome are higher. If a tibial shortening is done, shortening over an IM nail and prophylactic compartment release are recommended. We limit the use of shortenings to 4 to 5 cm leg length inequality in patients who are skeletally mature.
What Are Fallen Arches
Overview

Also sometimes called "fallen arches", the condition of flat feet is characterized by a lack of appropriate arch in the inner foot. It can be a genetic condition or the result of improper body mechanics. Often the whole of the foot will contact the ground with little to no arch being present. Because a normal foot is structurally able to support the weight of the body thanks to the bone structure that comprises the arch, a flat foot often is unable to properly support this weight and will cause extreme pressure in the joints in the foot and above, such as the ankles, knees and hips. Other problems such as tendonitis, bunion and hammertoe deformities, arthritis of the foot joints, and chronic fatigue of the leg muscles can also result.
Causes
Fallen arches have many causes. If you have fallen arches, or flat feet, the normal arch in the middle of your foot is not curved properly. You can have this condition called ples planus in medical terms and never have any symptoms. However, fallen arches can lead to foot pain, fatigue or more serious conditions. If fallen arches alter the way you walk, you may eventually develop knee, hip and low back pain. Your foot may lose normal range of motion making it hard to rise up onto your toes. In some cases, your feet can become swollen. If you have this condition, talk to your doctor about an appropriate treatment plan.
Symptoms
Flat feet may not cause any symptoms at all. Rigid flat feet may cause pain, calluses, blisters, or skin redness on the inner side of the foot. A stiff foot, weakness or numbness of the foot, Rapid wearing out of shoes-worn shoes lean in toward each other. Difficulty or pain with activities like running-in the foot, knee or hip.
Diagnosis
Many medical professionals can diagnose a flat foot by examining the patient standing or just looking at them. On going up onto tip toe the deformity will correct when this is a flexible flat foot in a child with lax joints. Such correction is not seen in the adult with a rigid flat foot. An easy and traditional home diagnosis is the "wet footprint" test, performed by wetting the feet in water and then standing on a smooth, level surface such as smooth concrete or thin cardboard or heavy paper. Usually, the more the sole of the foot that makes contact (leaves a footprint), the flatter the foot. In more extreme cases, known as a kinked flatfoot, the entire inner edge of the footprint may actually bulge outward, where in a normal to high arch this part of the sole of the foot does not make contact with the ground at all.
What is PES Planovalgus deformity?
Non Surgical Treatment
Custom orthotics are specially designed insoles, which are made for your by prescription. This is done by taking a plaster cast of the foot in its neutral position and is then sent to a laboratory, with your prescription to be made to your exact specifications. The insole then correctly aligns your foot and as a result your body. This will relieve abnormal strain of tissues and structures which can cause pain. For less severe mal-alignments or for sports use a wide variety of temporary insoles.
Surgical Treatment

In cases of flat feet that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required and in some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
Also sometimes called "fallen arches", the condition of flat feet is characterized by a lack of appropriate arch in the inner foot. It can be a genetic condition or the result of improper body mechanics. Often the whole of the foot will contact the ground with little to no arch being present. Because a normal foot is structurally able to support the weight of the body thanks to the bone structure that comprises the arch, a flat foot often is unable to properly support this weight and will cause extreme pressure in the joints in the foot and above, such as the ankles, knees and hips. Other problems such as tendonitis, bunion and hammertoe deformities, arthritis of the foot joints, and chronic fatigue of the leg muscles can also result.
Causes
Fallen arches have many causes. If you have fallen arches, or flat feet, the normal arch in the middle of your foot is not curved properly. You can have this condition called ples planus in medical terms and never have any symptoms. However, fallen arches can lead to foot pain, fatigue or more serious conditions. If fallen arches alter the way you walk, you may eventually develop knee, hip and low back pain. Your foot may lose normal range of motion making it hard to rise up onto your toes. In some cases, your feet can become swollen. If you have this condition, talk to your doctor about an appropriate treatment plan.
Symptoms
Flat feet may not cause any symptoms at all. Rigid flat feet may cause pain, calluses, blisters, or skin redness on the inner side of the foot. A stiff foot, weakness or numbness of the foot, Rapid wearing out of shoes-worn shoes lean in toward each other. Difficulty or pain with activities like running-in the foot, knee or hip.
Diagnosis
Many medical professionals can diagnose a flat foot by examining the patient standing or just looking at them. On going up onto tip toe the deformity will correct when this is a flexible flat foot in a child with lax joints. Such correction is not seen in the adult with a rigid flat foot. An easy and traditional home diagnosis is the "wet footprint" test, performed by wetting the feet in water and then standing on a smooth, level surface such as smooth concrete or thin cardboard or heavy paper. Usually, the more the sole of the foot that makes contact (leaves a footprint), the flatter the foot. In more extreme cases, known as a kinked flatfoot, the entire inner edge of the footprint may actually bulge outward, where in a normal to high arch this part of the sole of the foot does not make contact with the ground at all.
What is PES Planovalgus deformity?
Non Surgical Treatment
Custom orthotics are specially designed insoles, which are made for your by prescription. This is done by taking a plaster cast of the foot in its neutral position and is then sent to a laboratory, with your prescription to be made to your exact specifications. The insole then correctly aligns your foot and as a result your body. This will relieve abnormal strain of tissues and structures which can cause pain. For less severe mal-alignments or for sports use a wide variety of temporary insoles.
Surgical Treatment
In cases of flat feet that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required and in some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
What Causes Mortons Neuroma
Overview
 Morton's neuroma is an inflammation of the nerves in the foot that go to the toes. Although the name includes the word ?neuroma,? it is not really a tumor. It can affect any of the toes in the foot. However, it most often affects the nerves that run between the third and fourth, or second and third toes.
Morton's neuroma is an inflammation of the nerves in the foot that go to the toes. Although the name includes the word ?neuroma,? it is not really a tumor. It can affect any of the toes in the foot. However, it most often affects the nerves that run between the third and fourth, or second and third toes.
Causes
Various factors have been implicated in the precipitation of Morton's neuroma. Morton's neuroma is known to develop as a result of chronic nerve stress and irritation, particularly with excessive toe dorsiflexion. Poorly fitting and constricting shoes (ie, small toe box) or shoes with heel lifts often contribute to Morton's neuroma. Women who wear high-heeled shoes for a number of years or men who are required to wear constrictive shoe gear are at risk. A biomechanical theory of causation involves the mechanics of the foot and ankle. For instance, individuals with tight gastrocnemius-soleus muscles or who excessively pronate the foot may compensate by dorsiflexion of the metatarsals subsequently irritating of the interdigital nerve. Certain activities carry increased risk of excessive toe dorsiflexion, such as prolonged walking, running, squatting, and demi-pointe position in ballet.
Symptoms
A Morton's neuroma causes a "burning" sharp pain and numbness on the bottom of the foot in the involved area, and this pain and numbness can radiate to the nearby toes. The pain is usually increased by walking or when the ball of the foot is squeezed together and decreased with massaging. It may force a person to stop walking or to limp from the pain.
Diagnosis
Diagnosis of Morton?s Neuroma typically involves a physical examination of the affected foot. Your health care provider will ask you about your symptoms and examine your feet and toes. He will manipulate your toes, pushing them from side to side and squeezing on the spaces in between. This physical exam will allow your health care provider to feel for any lumps that may be present under the soft tissue of your feet. Your health care provider may also listen for any clicking sounds that your bones may be making. Known as Muldor?s Sign, this clicking is common amongst sufferers of foot neuroma. Occasionally, an x-ray or MRI (magnetic resonance imaging) is performed to help rule out any breaks, sprains, or fractures in your foot.
Non Surgical Treatment
There are various options for treating the condition, depending on its severity. Self-treatment. Here are some simple steps that may improve symptoms. Wear supportive shoes with a wide toe box. Do not lace the forefoot of the shoe too tightly. Shoes with shock-absorbent soles and proper insoles are recommended. Do not wear tight or pointed toed shoes or shoes with heels more than 2 inches high. Use over-the-counter shoe pads to relieve pressure. Apply an ice pack to the affected area to reduce pain and swelling. Rest your feet and massage the painful area. There are drugs that may temporarily relieve the pain and other symptoms of Morton?s neuroma. Long-term use of these medications is not recommended. Anti-inflammatory drugs-Nonsteroidal anti-inflammatory drugs, such as ibuprofen or aspirin, may be taken orally to reduce pain and inflammation. Anti-inflammatory drugs can also be administered by direct injection into the skin. Local anesthetic. An anesthetic injection will temporarily relieve pain by numbing the affected nerve. Orthotics. These are custom-designed shoe inserts that can reduce some of the pain associated with Morton?s neuroma. Sometimes padding is placed around the toe area, and tape is applied to hold the padding in place.
Surgical Treatment
Majority of publications including peer review journal articles, surgical technique description and textbooks promote surgical excision as a gold standard treatment. Surgical excision is described as the most definitive mode of treatment for symptomatic Morton?s neuroma with reported success rates varying between 79% and 93%. Various surgical techniques are described, essentially categorised as dorsal versus plantar incision approaches. Beyond this the commonest technical variation described as influencing the outcome of surgery involves burying and anchoring transacted nerve into soft tissue such as muscle.
Prevention
To help reduce your chance of developing Morton's neuroma avoid wearing tight and/or high-heeled shoes. Maintain or achieve ideal body weight. If you play sports, wear roomy, properly fitting athletic footwear.
Morton's neuroma is an inflammation of the nerves in the foot that go to the toes. Although the name includes the word ?neuroma,? it is not really a tumor. It can affect any of the toes in the foot. However, it most often affects the nerves that run between the third and fourth, or second and third toes.Causes
Various factors have been implicated in the precipitation of Morton's neuroma. Morton's neuroma is known to develop as a result of chronic nerve stress and irritation, particularly with excessive toe dorsiflexion. Poorly fitting and constricting shoes (ie, small toe box) or shoes with heel lifts often contribute to Morton's neuroma. Women who wear high-heeled shoes for a number of years or men who are required to wear constrictive shoe gear are at risk. A biomechanical theory of causation involves the mechanics of the foot and ankle. For instance, individuals with tight gastrocnemius-soleus muscles or who excessively pronate the foot may compensate by dorsiflexion of the metatarsals subsequently irritating of the interdigital nerve. Certain activities carry increased risk of excessive toe dorsiflexion, such as prolonged walking, running, squatting, and demi-pointe position in ballet.
Symptoms
A Morton's neuroma causes a "burning" sharp pain and numbness on the bottom of the foot in the involved area, and this pain and numbness can radiate to the nearby toes. The pain is usually increased by walking or when the ball of the foot is squeezed together and decreased with massaging. It may force a person to stop walking or to limp from the pain.
Diagnosis
Diagnosis of Morton?s Neuroma typically involves a physical examination of the affected foot. Your health care provider will ask you about your symptoms and examine your feet and toes. He will manipulate your toes, pushing them from side to side and squeezing on the spaces in between. This physical exam will allow your health care provider to feel for any lumps that may be present under the soft tissue of your feet. Your health care provider may also listen for any clicking sounds that your bones may be making. Known as Muldor?s Sign, this clicking is common amongst sufferers of foot neuroma. Occasionally, an x-ray or MRI (magnetic resonance imaging) is performed to help rule out any breaks, sprains, or fractures in your foot.
Non Surgical Treatment
There are various options for treating the condition, depending on its severity. Self-treatment. Here are some simple steps that may improve symptoms. Wear supportive shoes with a wide toe box. Do not lace the forefoot of the shoe too tightly. Shoes with shock-absorbent soles and proper insoles are recommended. Do not wear tight or pointed toed shoes or shoes with heels more than 2 inches high. Use over-the-counter shoe pads to relieve pressure. Apply an ice pack to the affected area to reduce pain and swelling. Rest your feet and massage the painful area. There are drugs that may temporarily relieve the pain and other symptoms of Morton?s neuroma. Long-term use of these medications is not recommended. Anti-inflammatory drugs-Nonsteroidal anti-inflammatory drugs, such as ibuprofen or aspirin, may be taken orally to reduce pain and inflammation. Anti-inflammatory drugs can also be administered by direct injection into the skin. Local anesthetic. An anesthetic injection will temporarily relieve pain by numbing the affected nerve. Orthotics. These are custom-designed shoe inserts that can reduce some of the pain associated with Morton?s neuroma. Sometimes padding is placed around the toe area, and tape is applied to hold the padding in place.
Surgical Treatment
Majority of publications including peer review journal articles, surgical technique description and textbooks promote surgical excision as a gold standard treatment. Surgical excision is described as the most definitive mode of treatment for symptomatic Morton?s neuroma with reported success rates varying between 79% and 93%. Various surgical techniques are described, essentially categorised as dorsal versus plantar incision approaches. Beyond this the commonest technical variation described as influencing the outcome of surgery involves burying and anchoring transacted nerve into soft tissue such as muscle.
Prevention
To help reduce your chance of developing Morton's neuroma avoid wearing tight and/or high-heeled shoes. Maintain or achieve ideal body weight. If you play sports, wear roomy, properly fitting athletic footwear.
Are Shoe Lifts The Solution To Leg Length Difference
There are two different kinds of leg length discrepancies, congenital and acquired. Congenital means that you are born with it. One leg is anatomically shorter in comparison to the other. As a result of developmental phases of aging, the human brain picks up on the walking pattern and identifies some variance. Your body typically adapts by dipping one shoulder to the "short" side. A difference of under a quarter inch is not blatantly irregular, doesn't need Shoe Lifts to compensate and in most cases doesn't have a serious effect over a lifetime.

Leg length inequality goes mainly undiscovered on a daily basis, yet this condition is very easily solved, and can reduce a number of instances of chronic back pain.
Therapy for leg length inequality commonly involves Shoe Lifts. These are generally affordable, frequently being less than twenty dollars, compared to a custom orthotic of $200 plus. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Back ache is easily the most prevalent condition impacting men and women today. Around 80 million men and women have problems with back pain at some stage in their life. It's a problem that costs employers huge amounts of money yearly on account of time lost and production. Fresh and superior treatment methods are constantly sought after in the hope of reducing the economical influence this issue causes.

People from all corners of the earth experience foot ache due to leg length discrepancy. In most of these situations Shoe Lifts are usually of worthwhile. The lifts are capable of reducing any pain and discomfort in the feet. Shoe Lifts are recommended by numerous certified orthopaedic orthopedists.
So that you can support the body in a well balanced manner, your feet have got a critical function to play. Despite that, it is often the most overlooked area of the body. Some people have flat-feet which means there may be unequal force placed on the feet. This will cause other parts of the body like knees, ankles and backs to be affected too. Shoe Lifts make sure that ideal posture and balance are restored.
Leg length inequality goes mainly undiscovered on a daily basis, yet this condition is very easily solved, and can reduce a number of instances of chronic back pain.
Therapy for leg length inequality commonly involves Shoe Lifts. These are generally affordable, frequently being less than twenty dollars, compared to a custom orthotic of $200 plus. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Back ache is easily the most prevalent condition impacting men and women today. Around 80 million men and women have problems with back pain at some stage in their life. It's a problem that costs employers huge amounts of money yearly on account of time lost and production. Fresh and superior treatment methods are constantly sought after in the hope of reducing the economical influence this issue causes.
People from all corners of the earth experience foot ache due to leg length discrepancy. In most of these situations Shoe Lifts are usually of worthwhile. The lifts are capable of reducing any pain and discomfort in the feet. Shoe Lifts are recommended by numerous certified orthopaedic orthopedists.
So that you can support the body in a well balanced manner, your feet have got a critical function to play. Despite that, it is often the most overlooked area of the body. Some people have flat-feet which means there may be unequal force placed on the feet. This will cause other parts of the body like knees, ankles and backs to be affected too. Shoe Lifts make sure that ideal posture and balance are restored.
Is Hammer Toe Debilitating
 Overview
Overview
Hammertoe is a condition in which the toes of your feet become contracted into an upside-down "V" shape, causing pain, pressure and, often, corns and calluses. Hammer toe can develop on any of the toes, but generally affects the middle three toes, most often the second toe. The bones, muscles, ligaments and tendons of your feet normally are well-balanced to distribute your body's weight while standing, walking and running. When the first and second joints of your toes experience the prolonged stress that develops when the muscles that control them fail to work together properly, the pressure on the tendons that support them can lead to the curling or contraction known as hammertoe.
Causes
Hammer toe is often caused by wearing shoes that do not fit properly. If shoes are too small either in length or width, then the toes are held in a shortened position for long periods and the muscles eventually shorten and pull the toes into the bent position. Alternatively it can be caused by overactivity in the extensor digitorum dongus muscle (right) and a weakness in the counteracting muscle under the foot, such as flexor digitorum longus. Sometimes it can be a congenital condition, meaning it is present from birth. It is also more common in those with arthritis in the foot or diabetes.
 Symptoms
Symptoms
A hammer toe may be painful, especially when irritated by a shoe. All four toe conditions may cause cramps in the toes, foot and leg due to the abnormal function of the tendons in the foot. If a mallet toe has occurred, you are likely to suffer from a corn at the end of the toe. A hammertoe may cause a corn on the top of the toe. Infections and ulcers can also occur. In severe cases a mallet toe, trigger toe, claw toe or Hammer toes a hammer toe may create a downward pressure on the foot, which can result in hard skin and corns on the soles of the feet.
Diagnosis
The treatment options vary with the type and severity of each hammer toe, although identifying the deformity early in its development is important to avoid surgery. Your podiatric physician will examine and X-ray the affected area and recommend a treatment plan specific to your condition.
Non Surgical Treatment
In the earlier stages of hammer toe, when the toes can still be manually straightened, then conservative treatment is appropriate. This means wearing shoes which are a half size bigger than normal and which are not narrow around the toes. Exercises to stretch the toes out and strengthen the muscles under the foot which balances the tightness of the top tendons are important. Padding or corn plasters can be used to ease the discomfort of any associated corns and calluses.
Surgical Treatment
Extreme occurrences of hammer toe may call for surgery. Your surgeon will decide which form of surgery will best suit your case. Often, the surgeon may have to cut or remove a tendon or ligament. Depending on the severity of your condition, the bones on both sides of the joint afflicted may need to be fused together. The good news is you can probably have your surgery and be released to go home in one day. You will probably experience some stiffness in your toe, but it might last for a short period, then your long-term pain will be eliminated.
Hammer Toe Correction Surgery Procedure
 Overview
Overview
A Hammertoes is a toe that tends to remain bent at the middle joint in a claw-like position. There are 2 types of hammer toe. Flexible hammer toe, can be straightened by hand. Rigid hammer toe, cannot be pulled straight and can be extremely painful. The position of the toe can also lead to corns or calluses. These may also be painful. Hammer toe may be present at birth or develop later in life due to tendons that have tightened, causing the toe's joints to curl downward. Occasionally, all toes may be bent. This may be due to problems with the peripheral nerves or the spinal cord.
Causes
Shoes that narrow toward the toe may make your forefoot look smaller. But they also push the smaller toes into a flexed (bent) position. The toes rub against the shoe, leading to the formation of corns and calluses, which further aggravate the condition. A higher heel forces the foot down and squishes the toes against the shoe, increasing the pressure and the bend in the toe. Eventually, the toe muscles become unable to straighten the toe, even when there is no confining shoe. 
Symptoms
Symptoms may include pain in the affected toe or toes when you wear shoes, making it hard or painful to walk. A corn or callus on the top of the joint caused by rubbing against the shoe. Swelling and redness of the skin over the joint. Trouble finding comfortable shoes.
Diagnosis
The earlier a hammertoe is diagnosed, the better the prognosis and treatment options. Your doctor will be able to diagnose your hammertoe with a simple examination of the foot and your footwear. He or she may take an x-ray to check the severity of the condition. You may also be asked about your symptoms, your normal daily activities, and your medical and family history.
Non Surgical Treatment
Treatment for a hammertoe usually depends on the stage of the hammertoe and the cause of the condition. If your toe is still bendable, your doctor may suggest conservative care-relieving pressure with padding and strapping, or proper shoes that have a deep toe box and are of adequate length and width. Early intervention can often prevent the need for surgery.
Surgical Treatment
Surgery is the approach that is often necessary to correct hammertoe that fails to respond to nonsurgical management. Surgery is appropriate when the muscles and tendons involved in a hammertoe problem have become so tight that the joints are rigid, misaligned and unmovable. There are a number of surgical techniques for dealing with the complex range of joint, bone, muscle, tendon and ligament abnormalities that define each hammertoe's make-up. To correct a hammertoe deformity, the surgeon's goal is to restore the normal alignment of the toe joint, relieving the pressure that led to the hammertoe's development (this should also relieve the pain, as well). To do this, he or she may remove part of the boney structure that creates a prominence at the top of the joint. Tighten or loosen the muscles, tendons and ligaments around the toe joints. Realign the toe bones by cutting one or more and shifting their position, realigning muscles, tendons and ligaments accordingly. Use screws, wires or plates to hold the joint surfaces together until they heal. Reconstruct a badly damaged joint or replace it with an artificial implant.